The Translational Chasm: Why Most Drug Development Programmes Fail Despite Promising Early Data
When exceptional preclinical data meets catastrophic Phase II or Phase III failure — a deep analysis of the primary culprits behind drug development attrition and why early data so often paints a deceptively optimistic picture.
of drug candidates that enter human clinical trials will never reach the market. The journey from a promising screening hit to an approved therapeutic is fraught with scientific, financial, and regulatory landmines — and the most troubling failures arrive late.
Why does a molecule that cleanly eradicates tumours in a xenograft model, or reverses neurological deficits in a rodent, suddenly stall when introduced to human patients? The answer lies in a multi-faceted disconnect between controlled preclinical environments and the staggering biological complexity of human physiology.
What follows is an in-depth analysis of the primary culprits behind drug development attrition — and the emerging strategies being deployed to close the gap.
The Efficacy Cliff
Translational gap between animal models and human biological complexity.
Unforeseen Toxicity
Idiosyncratic DILI and cardiovascular off-target effects undetected preclinically.
PK / PD Disconnects
Flawed interspecies scaling of protein binding, tissue penetration, and clearance.
Chemistry Hurdles
Synthetic intractability and manufacturing costs at scale.
Advanced Models
Bridging the gap with organoids, organ-on-a-chip, and iPSC platforms.
Adaptive Trial Design
Statistical rescue through sample size re-estimation and biomarker enrichment.
In Silico Prediction
Localised AI for secure, high-parameter toxicity and PK modelling.
Formulation as PK Bridge
Re-engineering delivery to rescue molecules with poor systemic behaviour.

The Efficacy Cliff and the Translational Gap
It is estimated that 40–50% of late-stage drug failures are attributed to a fundamental lack of efficacy. The core of this issue is the translational gap — the physiological, genetic, and metabolic differences between animal models and humans.
A drug may exhibit perfect target engagement in a murine model but fail to produce the desired clinical outcome in humans. This happens for several interconnected reasons:
- Biological Complexity: Human diseases are rarely driven by a single, easily isolated pathway. A drug might successfully inhibit a specific kinase in a controlled assay, but in a human patient, compensatory biological networks and feedback loops rapidly bypass the blockade.
- Endpoint Mismatch: There is frequently a disconnect between the outcome measures used in animal pharmacology (e.g., changes in behaviour or biomarker expression) and the stringent clinical endpoints required by regulatory agencies (e.g., overall survival or significant symptom reduction).
- Target vs. Disease Pathology: The drug candidate successfully hits its biological target, but it transpires the target was a byproduct of the disease rather than its primary driver.
Unforeseen Toxicity and Safety Roadblocks
Whilst Phase I trials are designed to catch acute toxicities, chronic and idiosyncratic safety issues often remain hidden until the drug reaches larger, more diverse patient populations in Phase II and III. Standard in vitro and in vivo toxicological screenings are notoriously poor at predicting specific human adverse events. Two of the most common safety-related trial killers are:
Drug-Induced Liver Injury (DILI)
DILI is one of the leading causes of post-marketing withdrawal and late-stage trial termination. Conventional animal toxicology studies can typically detect intrinsic hepatotoxicity. However, they frequently fail to predict idiosyncratic DILI, which involves complex human immune and metabolic pathways that only manifest in a small fraction of susceptible populations.
Cardiovascular Toxicity
Prolongation of the QT interval and inhibition of the hERG potassium channel can lead to fatal ventricular arrhythmias. Because rodent cardiac electrophysiology differs significantly from humans, relying solely on traditional animal models can allow dangerous off-target effects to slip into human trials.
Pharmacokinetic (PK) and Pharmacodynamic (PD) Disconnects
A highly potent molecule is useless if it cannot reach its site of action at the right concentration for the right amount of time. Even with promising early data, flawed PK/PD scaling from animals to humans frequently derails programmes:
- Protein Binding and Free Drug Concentration: Preclinical data might show massive total drug concentrations in the blood, but if the drug is highly bound to human plasma proteins, the unbound fraction available to engage the target may be insufficient to drive a therapeutic effect.
- Tissue Penetration: Particularly problematic in CNS and solid tumour development — a drug might perform well in vitro but fail entirely because it cannot cross the blood-brain barrier or penetrate the dense stromal tissue of a tumour microenvironment.
- Metabolic Clearance Differences: A drug with a long half-life in a dog or monkey might be rapidly metabolised and cleared by human hepatic enzymes (such as the CYP450 system), preventing it from ever reaching a steady therapeutic state.
"Drug development does not fail for lack of biology. It fails at the interface between molecule, delivery, and human systems."
The "Synthesis Bottleneck" and Chemistry Hurdles
A phenomenon recently termed the "Oncology Paradox" highlights a unique reason for development failure. High-throughput screening and natural product isolation frequently yield incredibly complex, high-affinity molecules. Whilst these show great promise in early micro-dosing studies, scaling up their synthesis for large human trials reveals prohibitive costs and technical difficulties.
If a complex chemical scaffold cannot be optimised into a synthetically accessible, stable formulation, the clinical programme will bleed capital and eventually collapse under the weight of its own manufacturing demands.
Bridging the Gap: Advanced Humanised Models
The pharmaceutical industry is not standing still in the face of these failure rates. The passage of the FDA Modernization Act 2.0 has accelerated the adoption of alternative preclinical models. Several paradigm shifts are actively working to close the translational gap:
- Patient-Derived 3D Organoids: Allowing efficacy and safety testing on actual human tissue long before a Phase I trial begins.
- Microfluidic "Organ-on-a-Chip" Systems: Recapitulating human organ physiology with unprecedented fidelity, enabling mechanistic studies impossible in static cell culture.
- Induced Pluripotent Stem Cells (iPSCs): Providing genetically diverse human cell populations for idiosyncratic toxicity screening.
- Translatable Biomarkers: Developing biomarkers measurable identically across species to bridge nonclinical data directly to human outcomes via quantified exposure-response relationships.
The Biostatistical Rescue: Rigid vs. Adaptive Trial Designs
Often, a clinical trial fails not because the investigational product is ineffective, but because the trial's statistical architecture was too rigid. Traditional randomised controlled trials (RCTs) force researchers to lock in assumptions regarding effect size, control group event rates, and population variance years before the data is generated. If Phase II data slightly miscalculates these parameters, a genuinely efficacious drug might fail to reach statistical significance in Phase III.
To combat this, the FDA and EMA are increasingly encouraging Adaptive Clinical Trial Designs — statistical frameworks allowing pre-specified modifications to the trial based on accumulating interim data, without compromising integrity or inflating the Type I error (false-positive) rate. Key adaptive strategies include:
Sample Size Re-estimation
If an interim unblinded analysis reveals that outcome variance is higher than initially modelled, statisticians can dynamically recalculate and increase the sample size mid-flight to preserve the trial's statistical power.
Biomarker Enrichment
If early data indicates the drug is predominantly effective in a specific genetic or biomarker-positive subpopulation, the trial can adapt to restrict future enrolment exclusively to that cohort — preventing the drug's true efficacy from being diluted by non-responders, and turning a potential overall failure into a targeted success.
In Silico Prediction and the Rise of Localised AI
The pharmaceutical industry is moving aggressively to predict clinical failure before a molecule ever leaves the discovery phase. The current paradigm is shifting from broad machine learning models towards secure, high-parameter predictive modelling to map human-specific toxicities with far greater resolution.
Because proprietary pharmacophores and unpatented drug structures are highly sensitive, reliance on public cloud AI is often a non-starter. Instead, deploying a robust local AI platform allows research teams to securely process massive volumes of journal articles, parse historical clinical trial data, and run predictive toxicology models entirely in-house.
Deploying a localised AI platform such as SynapTx™ enables research teams to securely analyse massive pharmacokinetic datasets to predict human clearance rates, map complex metabolic profiles, and flag potential idiosyncratic liver injuries (DILI) that animal models routinely miss — entirely within a secure, proprietary environment.
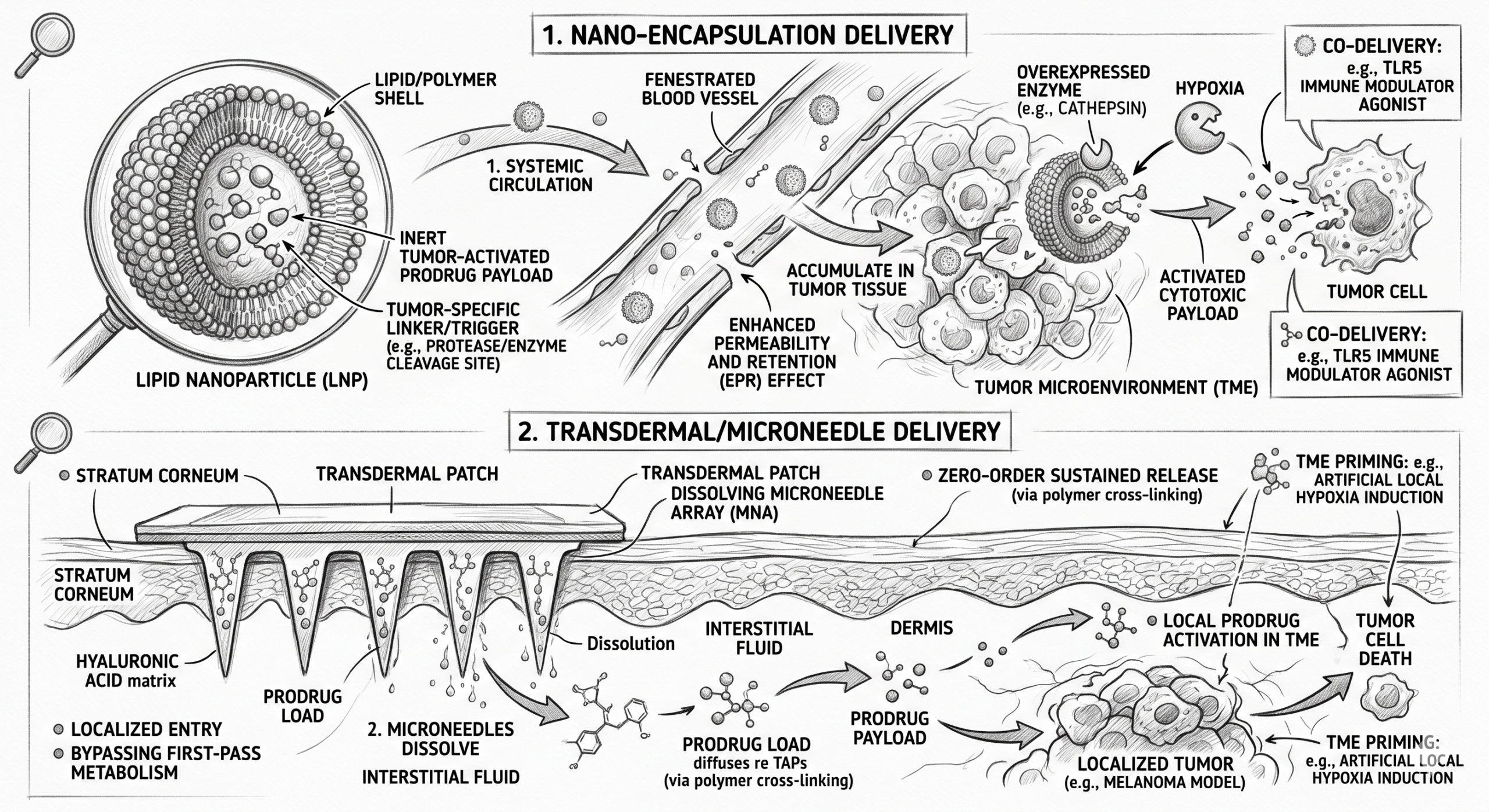
Formulation as a Pharmacokinetic Bridge
When a drug fails in early trials due to a poor PK/PD profile — an excessively short half-life, poor oral bioavailability, or severe peak-to-trough fluctuations causing dose-limiting toxicities — the default response has historically been to abandon the molecule entirely.
Advanced formulation science is increasingly deployed to rescue these "failed" candidates. Rather than returning to the computationally expensive discovery phase, scientists can re-engineer the delivery mechanism to manipulate the drug's systemic behaviour:
| Approach | Mechanism & Rationale |
|---|---|
| Bilayer & Multi-Particulate Tablets | For drugs requiring high sustained concentrations but subject to rapid clearance, bilayer formulations deliver an immediate-release loading dose to saturate hepatic enzymes — seamlessly followed by a sustained-release matrix that maintains steady-state therapeutic levels. |
| Delayed-Release Systems | If a drug fails Phase I due to severe gastrointestinal distress or high acid lability, targeted enteric coatings bypass gastric degradation entirely — releasing the active pharmaceutical ingredient (API) precisely in the alkaline environment of the duodenum or jejunum. |
The most valuable shift in modern drug development is not a single technology — it is the discipline of addressing failure points systematically and early. Integrating predictive modelling, adaptive trial architecture, and formulation engineering into a unified development strategy is no longer a competitive advantage; it is the minimum viable approach for a programme with serious clinical ambition.